Researchers at the Wayne State University School of Medicine and the National Institutes of Health’s Perinatology Research Branch in Detroit have discovered that the more severely infected with COVID-19 a mother is, the more likely she is to experience preterm birth.
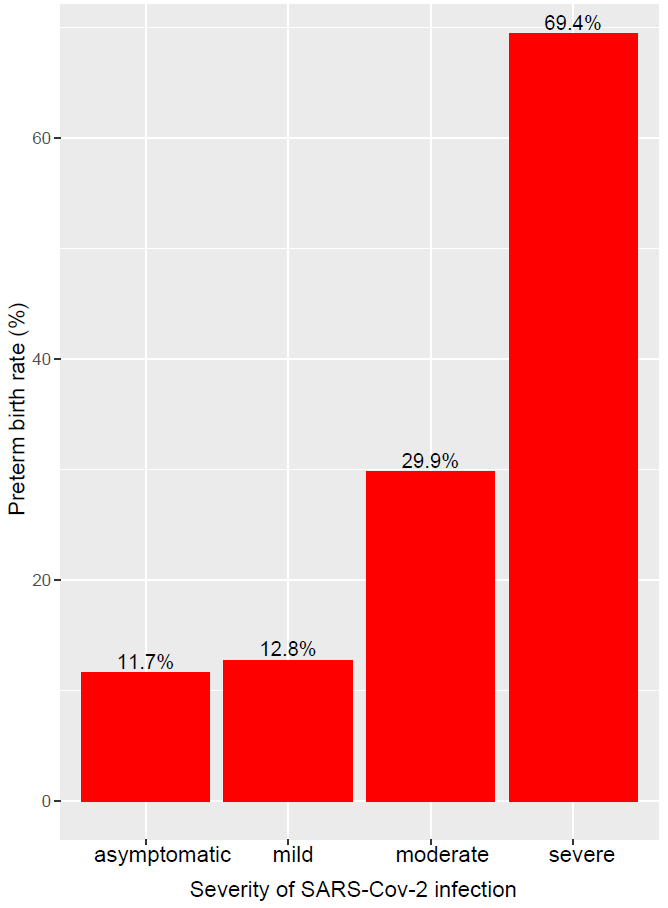
In “SARS-CoV-2 and the subsequent development of preeclampsia and preterm birth: evidence of a dose response relationship supporting causality,” published in the American Journal of Obstetrics and Gynecology, the researchers reported that the rate of preterm birth in about 1,000 pregnant women who tested positive for SARS-CoV-2, the virus that causes COVID-19, was a function of the severity of infection.
“The more severe the SARS-CoV-2 infection, the greater the risk of preterm birth,” said Roberto Romero, M.D., DMedSci, chief of the Perinatology Research Branch and professor of Molecular Obstetrics and Genetics at the Wayne State University School of Medicine. “There was a dose-dependent relationship between the severity of SARS-CoV-2 infection and the risk of prematurity.”
The WSU/PRB researchers conducted the study in collaboration with the Fetal Medicine Foundation of London, finding that the rate of preterm birth in about 1,000 pregnant women who tested positive for COVID-19 depended on the severity of their infection. The excess rate of premature birth, they report, is largely due to medically-induced preterm birth brought about by concerns for the health of the mother, such as preeclampsia.
Preterm birth, the leading cause of perinatal morbidity and mortality worldwide, is defined as one that occurs before 37 weeks of gestation. Two-thirds of preterm births are due to spontaneous onset of preterm labor. The remaining third is due to medical conditions that affect either the mother or the unborn baby that necessitate delivery.
The more severe the COVID-19 infection, the greater the risk of preeclampsia, a sudden increase in blood pressure after the 20th week of pregnancy. The condition is responsible for 76,000 maternal deaths and more than 500,000 infant deaths every year. Some mothers develop seizures (eclampsia) and suffer intracranial hemorrhage, the main cause of death in those who develop the disorder. Some women develop blindness. The babies of preeclamptic mothers are affected by the condition and may develop intrauterine growth restriction or die in utero.
Doctors appear to be medically inducing early delivery to save the lives of mothers infected with COVID-19 in the cohort studied.
Regardless of those medically induced preterm births, the researchers said, the possibility that COVID-19 infection causes preeclampsia must be considered.
“The principal finding is that there is a dose-response relationship between the severity of SARS-CoV-2 infection and the risk of subsequent development of preeclampsia and preterm birth,” Dr. Romero said. “Patients with severe COVID-19 have a five-fold greater risk of preeclampsia than asymptomatic patients. Moreover, the relative risk of developing preeclampsia in women with moderate or severe COVID-19 was 3.3-fold higher than in those with asymptomatic or mild infection.”
In addition to Dr. Romero, the research team included Adi Tarca, Ph.D., professor of Obstetrics and Gynecology, and adjunct professor of Computer Science at Wayne State University and a member of the PRB; Jonathan Lai, M.D., Fetal Medicine Research Institute, King’s College Hospital, London; Stamatina Iliodromiti, M.D., Centre for Women’s Health, Institute of Population Health, Queen Mary University of London, London; Anoop Rehal, M.D., Department of Obstetrics and Gynaecology, Birmingham Heartlands Hospital, Birmingham, West Midlands; Anita Banerjee, M.D., Women’s Services Department, St. Thomas’ Hospital, London; Christina Yu, M.D., Department of Fetal Medicine, St. Mary’s Hospital, Imperial College National Health Services Trust, London; Gergana Peeva, M.D., Department of Fetal Medicine, Homerton University Hospital, London; Vadivu Palaniappan, M.D., Department of Obstetrics and Gynaecology, Queen Elizabeth Hospital, London; Linda Tan, M.D., Department of Obstetrics and Gynaecology, University Hospital Lewisham, London; Mahishee Mehta, M.D., Department of Obstetrics and Gynaecology, Northwick Park Hospital, London; and Kypros Nicolaides, M.D., Fetal Medicine Research Institute, King’s College Hospital, London.
This research was supported by a grant from the Fetal Medicine Foundation (charity no: 1037116 ). In addition, this research was supported, in part by the Perinatology Research Branch, Division of Obstetrics and Maternal-Fetal Medicine, Division of Intramural Research, Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Institutes of Health, U.S. Department of Health and Human Services; and in part with federal funds from NICHD/NIH/DHHS under contract no. HHSN275201300006C.